Tag: Allergy
-

Fibermaxxing Is Everywhere. Can It Actually Help Your Allergies?
Fibermaxxing is an emerging trend where individuals increase their fiber intake for potential health benefits, including better digestion and improved gut health. While many Americans consume insufficient fiber, the trend should not replace proven allergy treatments or medications. Gradually increasing fiber intake, with attention to dietary choices, can enhance metabolic health without curing food allergies.
-

How AlphaFold AI Is Changing the Future of Allergy Care
AlphaFold is an AI system by Google DeepMind that predicts protein shapes, enhancing research in molecular interactions critical for understanding allergies. It could enable more targeted allergy treatments by identifying key protein structures, but further validation is necessary. Although promising, patients should not rely solely on this technology for immediate solutions.
-
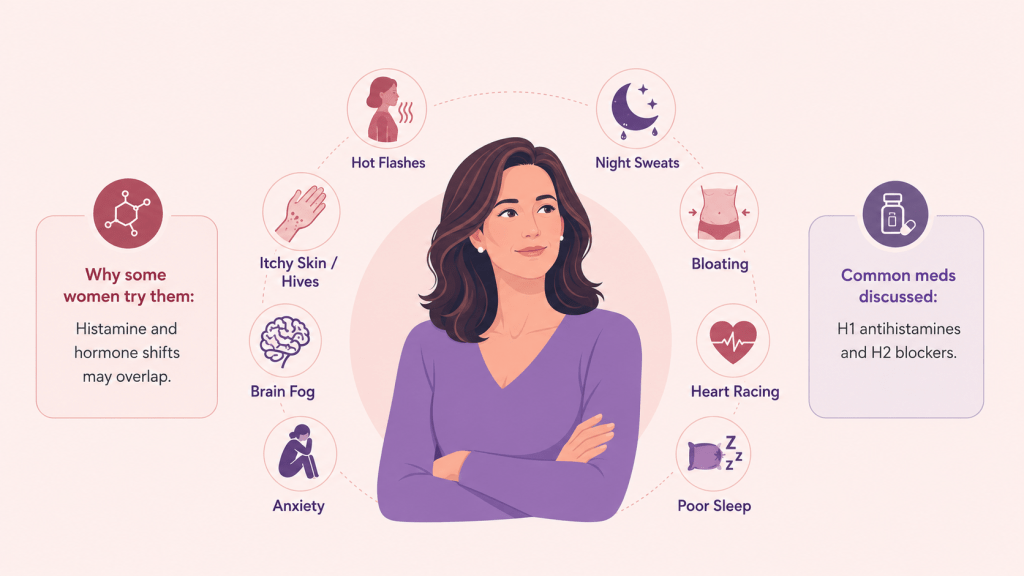
Why Are Women Taking Allergy Medications for Perimenopause Symptoms?
Many women experiencing perimenopause are using allergy medications to alleviate symptoms such as hot flashes and bloating, believing they may reduce hormone-related discomfort. While the connection between histamine and hormones is acknowledged, caution is advised due to the lack of clinical evidence for these treatments. Tracking symptoms and consulting a doctor is essential.
-
How Organic Foods, Conventional Foods, and Food Dyes Affect Allergies
The article discusses the impact of organic versus conventional foods on allergies, emphasizing that while organic dairy shows promise in reducing eczema risk, more research is needed to support sweeping conclusions. It also highlights concerns about pesticide exposure in conventional produce and the recent national focus on phasing out synthetic food dyes, encouraging gradual diet…
-
Could We “Turn Off” Allergies With Gene Editing? Here’s What CRISPR Actually Makes Possible
A baby with a fatal metabolic disorder was successfully treated with CRISPR gene editing, raising hopes for managing allergies. However, allergies involve complex genetic and environmental factors, making CRISPR a challenging solution. The future may include targeted treatments for immune disorders, but widespread applicability for allergies remains uncertain and ethically debated.
-
Peanut Patches and AI Food Allergen Detectors: Cures for Food Allergies?
Recent advancements in food allergy technology include a peanut patch and portable allergen scanners. While these tools show promise, they have limitations in their effectiveness. Serious reactions often occur in restaurants, and traditional strategies like oral immunotherapy provide stronger protection. Effective management still relies on careful avoidance, communication, and preparedness.
-

California Is Forcing Restaurants to Disclose Allergens. Here are the Risks Nobody Is Talking About.
California’s new restaurant allergen disclosure law starts July 1. For most people with food allergies, they will hear that and think, “Finally, I can relax when I eat out.” Unfortunately, it’s not so simple. And for non-Californians, just know that the Golden State is often the testing ground for food policy. If this law works,…
-

Spring Sneezes Are Starting Earlier Every Year. Here’s What That Means for You:
Spring allergy symptoms are starting earlier each year, with increased pollen counts leading to severe discomfort. To prepare, begin using nasal steroid sprays early, track local pollen levels, and maintain a clean indoor environment. Allergy shots can help reduce long-term sensitivity. Effective preparation can significantly improve the spring experience.
-
How Weight-Loss Drugs and AI Are Reshaping Allergy Medicine
In 2026, GLP-1 drugs and AI are transforming allergy care. While GLP-1 medications alter appetite signaling and aid weight loss, the potential for allergic reactions complicates patient experiences. AI enhances diagnostics by streamlining processes and improving accuracy, ultimately leading to better outcomes and fewer misdiagnoses in allergy treatments.
-

Women, Hormones, and Allergies: Why Your Symptoms Change and What to Do About It
Allergies exhibit different patterns in women and men, largely influenced by hormones. After puberty, estrogen increases allergy risk, causing symptoms tied to menstrual cycles and pregnancy. Understanding hormonal patterns can help women manage these flares with proactive treatment strategies, rather than reactive responses, improving overall quality of life through various life stages.
