Tag: Allergy
-

Hidden Allergens in the Home: What’s Really Irritating Your Body
Allergies are often underestimated as indoor problems, with volatile organic compounds (VOCs) and mold being significant irritants. VOCs are released from everyday items like carpets and electronics, while mold proliferates in HVAC systems. Both contribute to chronic respiratory issues, prompting the need for effective measures to improve indoor air quality and humidity management.
-

The Seed Oil–Allergy Link No One’s Explaining Correctly
Seed oils face criticism as a potential cause of health issues like inflammation and allergies. However, not all seed oils are harmful; those high in omega-6 fats can increase allergic sensitivity, while omega-3-rich oils can help reduce it. Making informed choices can significantly impact health and allergy symptoms over time.
-
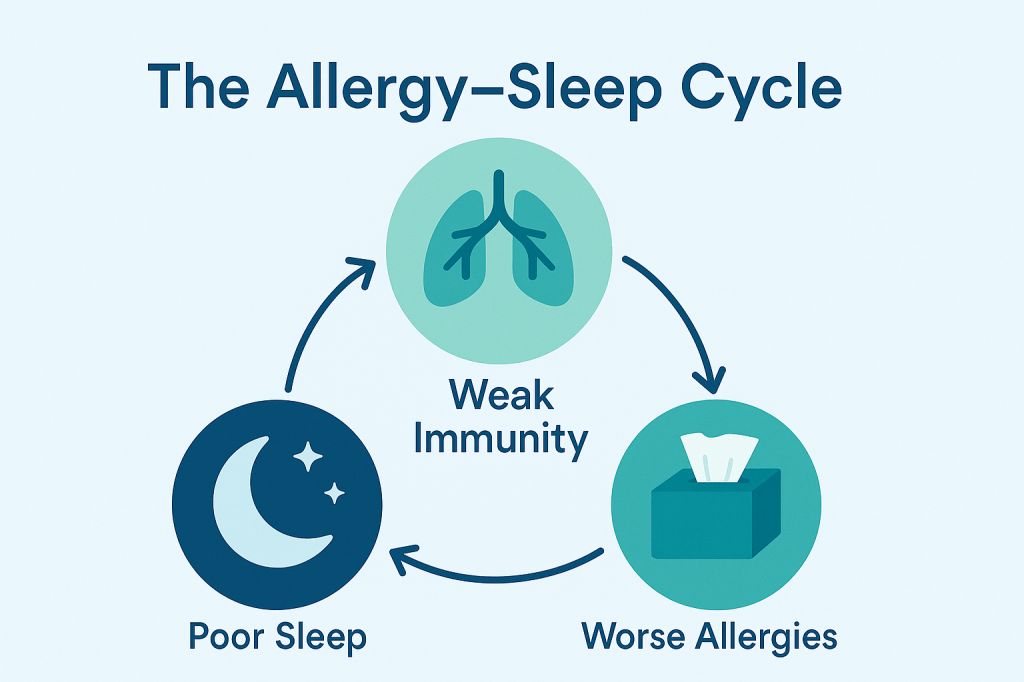
The Overlooked Connection Between Sleep and Allergies
Many overlook the link between sleep and allergies, but poor sleep can worsen allergic symptoms and overall immune function. Poor sleep leads to increased inflammation and allergic reactions. Improving sleep hygiene can alleviate allergy symptoms significantly, emphasizing the importance of prioritizing restful sleep as a key component of allergy management.
-

Hidden Allergens in Popular Diets: What You’re Overlooking (and How to Fix It)
The shift toward diets like keto, vegan, and paleo introduces hidden allergens that can pose serious risks. Reformulations in packaged foods, cross-contact during food preparation, and mismanagement of allergies complicate safety. It’s essential to be vigilant about ingredient changes and maintain a food diary to distinguish between true reactions and dietary adjustments.
-

The Overlooked Link Between Obesity and Allergies
When people talk about obesity, the conversation almost always stops at diet and exercise. Calories in, calories out. Move more, eat less. But here’s what almost no one mentions: obesity throws your immune system into overdrive. Every 5-point increase in BMI raises asthma risk by about 30%, and obese patients report worse control, more flare-ups,…
-

The Allergy Crisis No One in Public Health Wants to Talk About
Allergy rates have risen dramatically in the past 30 years, largely due to the hygiene hypothesis, which limits immune system exposure to microbes. Climate change also worsens allergies, while socioeconomic factors complicate the issue. Public health efforts prioritizing education, local pollen counts, and preventive measures could significantly reduce allergy-related healthcare costs and improve outcomes.
-

The Future of AI in Allergy Care: How It’s Already Changing Everything
AI is revolutionizing allergy care by significantly reducing the time allergists spend on documentation and enhancing diagnosis support. It improves the accuracy of medical records, enriches patient visits, expedites pre-screening, and streamlines business operations. Although AI augments physicians’ capabilities, human oversight remains crucial, paving the way for more personalized patient care.
-

The 7 Mistakes I Made Early in My Allergy Practice—And What I Do Differently Now
I’ll be honest: I built my allergy practice by stumbling first. I overpaid hospitals, underpriced visits, and clung to old protocols long after the data moved on. Here is the short version so you can skip the bruises—what I did wrong, what I do now, and the simple steps to copy this week. 1. I…
-

The Biggest Breakthroughs in Allergy Research This Year
Most allergy treatments still play defense. You react, you medicate, and then you wait for it to come back. But this year? We’re finally playing offense. From food allergies to eczema to asthma, the latest breakthroughs are revolutionizing the entire field. Here’s what’s new and what you can do about it right now. 1. Biologics…
-

The Top Allergy Triggers Lurking in Your Medicine Cabinet
Your medicine cabinet may contain allergy triggers, including leftover antibiotics, over-the-counter pain relievers like ibuprofen, topical creams, and inactive ingredients. Reactions can be immediate or delayed. Always use familiar medications, avoid sharing, and consult an allergist if you experience symptoms. Regularly clean and organize your cabinet for safety.
